
Berlin, Germany (Weltexpress). Dedicated to my wife Margaret Elizabeth Cook (1925-2018, who died while making this article. 65 years ago, I noticed how a certain pair of brown eyes glowed and twinkled in the evening sun. 55 years ago, I asked their owner to marry me. She said ‘Yes’ – and gave me three sons.
‘… an English unofficial rose’
“She had lived 93 loving years.”
“… the universality of an opinion is no proof,
nay, it is not even a probability,
that the opinion is right.”
(Arthur Schopenhauer, The Art of Controversy)
Summary
Evidence suggests that removal of the bit offers a solution for a wide range of health, welfare and safety problems currently besieging horse sports worldwide. This evaluation uses racing as an example of problems caused by the bit but the evidence applies to all disciplines.
Published last year, data on the effect a bit has on horse behavior showed that bit-induced pain was common. Also published recently, a comprehensive review concluded there was a “potential for ridden horses to experience three forms of breathlessness; unpleasant respiratory effort, air hunger and chest tightness.” These publications point to the likelihood that pain and suffocation are factors relevant to the cause of palatal instability, premature fatigue, poor performance, ‘bleeding’, catastrophic injuries and sudden death in the racehorse. Inevitably, these problems for the racehorse also affect the health and safety of exercise riders and jockeys. Though the extremes of horseracing’s problems may not affect other equestrian disciplines to the same extent, undoubtedly all disciplines are affected to varying degrees. Just as advances in motor car design have often had their origin in motor racing, a consideration of horseracing’s problems needs to be recognized as also relevant to endurance, eventing, dressage, pony club competitions and the whole of horsemanship.
Data on bit-induced suffocation has yet to be compiled. However, based on how a horse runs when at liberty (with sealed lips, closed mouth, extended head and neck, and unrestrained head-bob) it is already evident that the bit causes suffocation. The assumption can be rigorously tested, in due course, by measuring blood gas levels in bitted and bit-free horses at exercise.
In the meantime, the application of existing knowledge does not have to wait upon ‘more research’ or a change in the rules. Today’s knowledge can be applied now to the training of horses even though a bit is still required for competition. For example, dispensing with the bit when training a racehorse, – even if this can only be done for a few days each week – will itself further test the above prediction.
Until the rules are changed to allow bit-free racing, the prediction cannot be tested – under racing conditions – that removal of the bit will not only reduce pain but also the above consequences of suffocation. Nevertheless, pain reduction alone is sufficient reason for a trial rule change. If only one racing jurisdiction were to withdraw the rule mandating use of a bit, even for a probationary period, this would allow crucial performance figures and other evidence to be collected. Until the updating of rules mandating bits, current rules will continue to bar the trial of a potential solution to health, welfare and safety problems. In the meantime, the social license of horseracing itself remains at risk.
Horseracing is only a special case of a general problem in equitation; use of a bit. There is also a bit-shaped ‘elephant in the room’ of dressage, pony club competitions and any other horse sport for which a bit is mandated.–
Part I: The Problem
A Paulick Report headline caught my attention on the day before the 2018 Breeders’ Cup: “Mendelssohn Well-Behaved while ‘Stretching His Legs’ before Cigar Mile.” The headline captures trainers’ relief when a horse does not ‘run his race’ on the day before a valuable race is run. Unfortunately, the very steps taken to prevent a horse overexerting itself in a workout may have unintended consequences. The image at https://www.paulickreport.com/news/thoroughbred-racing/mendelssohn-well-behaved-while-stretching-his-legs-before-cigar-mile/ illustrates some warning signs (Fig.1).

Mendelssohn, the composer, wrote ‘Songs Without Words’ and Mendelssohn the horse is caught on camera exhibiting behavioral ‘Signs Without Words’. The image prompts me to ask the question: Why not consider ‘Races Without Bits’? Racing’s administrators will probably answer by asserting that a bit is indispensable for control and safety (but see the Schopenhauer quote above and the caption to Fig.2). On the contrary, evidence suggests that the bit may be the most common cause of loss of control (Cook and Kibler, 2018a). As for safety, a bit can deliver the unkindest cut of all. Bits can kill. A metal bit has been a customary part of a bridle since the Bronze Age but my studies in the last 20 years tell me that this custom is unkind and unnecessary, as the success of its primary purposes (control and safety) is challenged by evidence.

Mendelssohn’s equipment includes an eggbutt snaffle, tongue-tie, bit lifter and running martingale. The rider is taking ‘a strong hold.’ Mendelssohn’s negative behavioral signs include:
- flexure at the poll
- martingale preventing head/neck extension
- jowl angle judged to be less than 90o
- skin of neck creased behind the jaw
- throat airway bent and pinched
- open mouth
- stretched and unsealed lips
- retracted tongue
- excessive salivation
- ear positions asymmetric
The possible consequences include pain, suffocation, fatigue, and emotional stress for a horse; heightened risk of accident and injury for horse and rider; and racing success potentially denied for owner and trainer.
Pain
The signs indicate that Mendelssohn is experiencing oral pain from bit pressure on bone, tongue, lips and teeth.
- Bone: Gum is the outer sheath of the jawbone. This soft, strong and elastic ‘cushion’ is a specialized form of periosteum that functions to embed teeth into the jawbone and to provide the bone with blood, nutrients and nerve endings. The exquisitely sensitive ‘soft bone’ is highly vulnerable to bruising and its long-term consequences; i.e., bone-spur formation, osteomyelitis and, occasionally, the actual shedding of dead bone. We would experience severe pain if someone persistently pressed a thin metal rod against either of our shinbones. Yet the bars of a horse’s mouth, the ‘cushioned’ interdental space between the front teeth and the cheek teeth, are probably more sensitive than our own or a horse’s shins. The two bone ‘bars of the mouth’ are akin to a pair of ‘rails’, each with a knife-edge (Figs.3a and b). Strict avoidance of direct pressure on bone is a recognized requirement when fitting a saddle (Fig. 4). Yet this is not just flouted by fitting a bit, it is mandated. Thus, a horse being ‘on the bit’ and a rider having ‘contact’ are lauded as commendable goals of horsemanship.
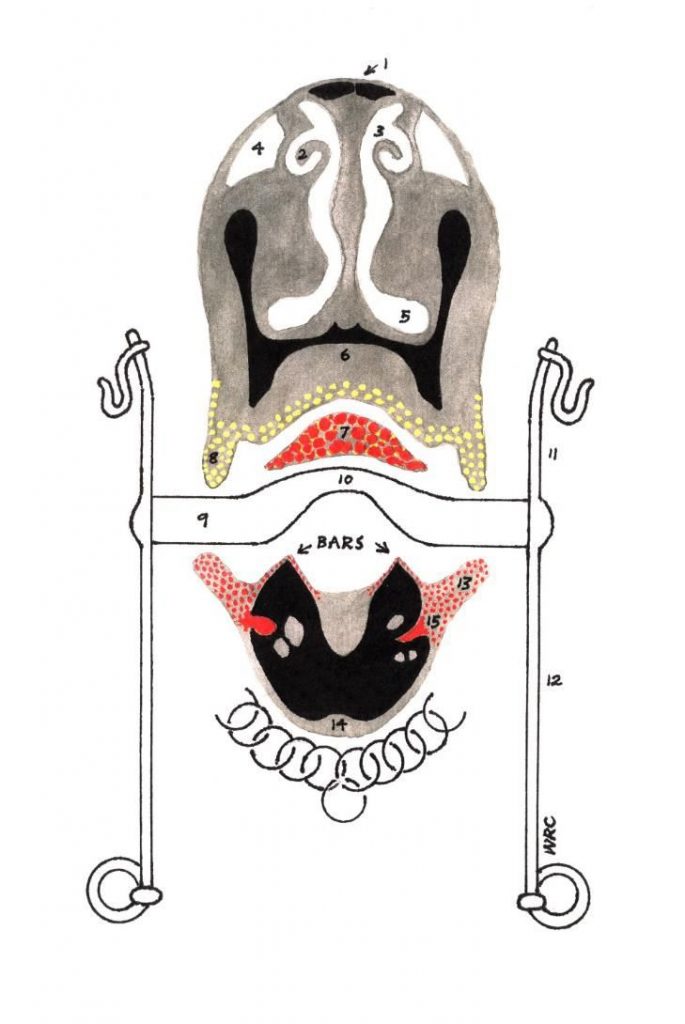
Key: black = bone; other colors = soft tissue; 1 = peak of nasal bone; 2 = nasal scroll; 3 = minor nasal airway; 4 = false nostril; 5 = major nasal airway; 6 = hard palate; 7 = tip of tongue; 8 = upper lip and roof of mouth; 9, 10 = mouthpiece of curb bit; 11, 12 = cheekpiece andshanks of curb; 13 = lower lip and gum; 14 = jawbone; 15 = sensory nerve


- Tongue: This sense organ is highly sensitive to thermal, chemical, mechanical and painful stimulation. A bit can bruise, cut and amputate the tongue or render it ‘blue’ from a curtailed blood supply. These various stimuli are all very likely to cause pain.
- Lips: Guardians of the ‘gate’ to the digestive tract, lips are an especially sensitive (whiskered) part of another sense organ, the skin. In Figure 1, the bit is acting as a lip retractor, stretching the already opened lips to their uttermost length. Anyone who has sat in a dentist’s chair and experienced this for 5 seconds will know how a horse may feel.
- Cheek teeth: Dental damage from the bit can be extensive, serious and very painful (Fig.2). Whether or not Mendelssohn is experiencing toothache as well as bone ache at the moment depicted in Figure 1 cannot be proven but the body language indicates that it is likely. A survey of 66 jawbones in four USA natural history museums revealed that 62% showed bone spur formation on the bars of the mouth and 61% showed erosion of the first lower cheek tooth (Cook 2010). In a few specimens, the first cheek tooth had been completely extracted by the bit.
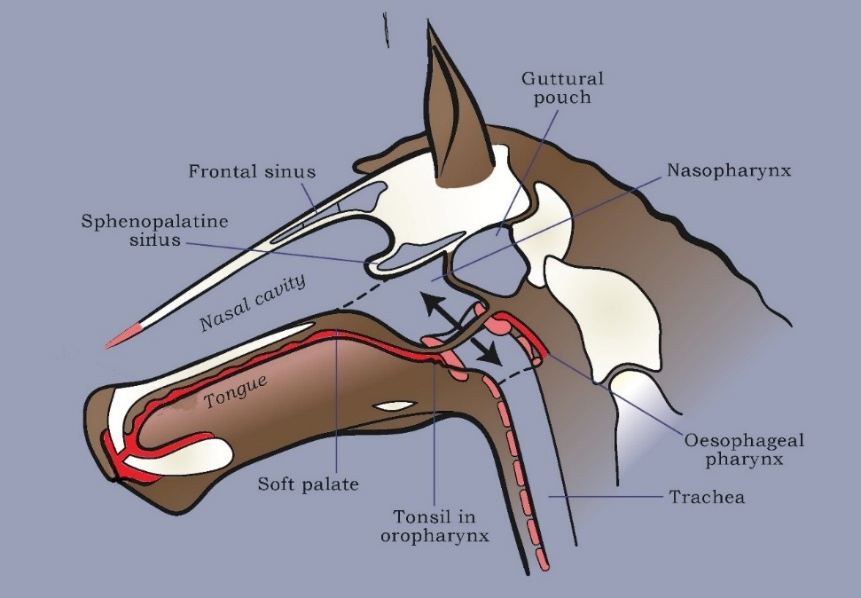
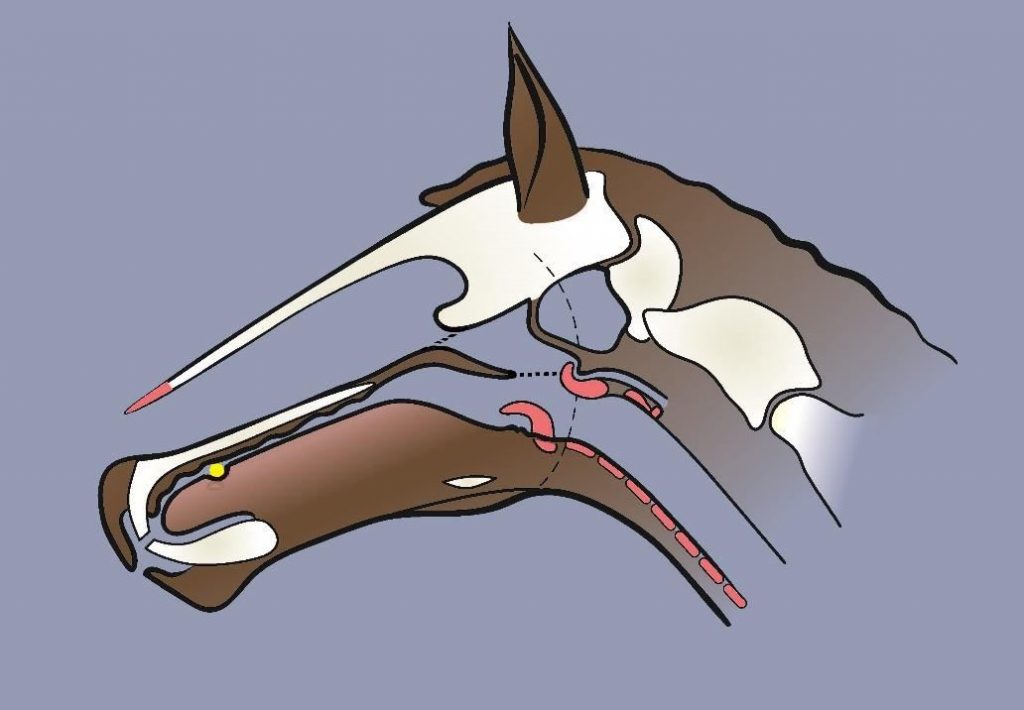
- Canine teeth: This is an overlooked item relevant to all male horses and some females. The anatomical name for the bars of a horse’s mouth is the ‘interdental space.’ Though the visible crown of the canine tooth when present breaks the continuity of the interdental space, the name of the space tempts us to think of it as ‘toothless.’ Yet, it is indisputably ‘dental.’ That portion of the space along which the bit painfully presses (i.e., that between the visible crown of the canine tooth and the first cheek tooth) contains the unerupted (‘reserve’) crown and (in old age) the root of the canine tooth (Figs. 3, 4, 5). We have unconsciously tended to assume that the reserve crown of the lower canine lies perpendicular to the long axis of the jaw (i.e., free of the bars) when, in fact, it lies parallel to and directly under the bars (Fig.5).

A bit can erode the erupted crown of the canine tooth but the location of its horizontally-located and unerupted reserve crown has been overlooked. In old age, there will also be a small root. It is bad enough that a bit painfully presses on bone but even worse when the bone is the socket of an actively erupting tooth. As canine teeth do not become visible (i.e., erupt through the gum) until a horse is about four years of age, they are actively developing (still entirely subgingival and within the socket) during the most critical years of a Thoroughbred’s racing career. Mendelssohn’s canine teeth, at five, will have been visible for about a year but they will still be growing. As with horses of all ages except old age (when a root finally forms and growth stops), horse’s teeth develop and continue to erupt during most of their life. It may be no coincidence that ‘headshaking,’ a behavioral sign of pain, shows a gender bias for being more common in male horses (Cook 2010, Cook and Kibler 2018).
- Wolf teeth: Vestigial first premolar ‘milk’ teeth are less common in the lower jaw than the upper. However, as bit pressure is predominantly confined to the lower jaw, wolf teeth in the lower jaw may be more consequential when present than those in the upper jaw, especially so when they are unerupted and invisible.
The phrase ‘a properly-fitted bit’ is an oxymoron; like the phrase ‘a definite maybe.’ Some horses fight the bit, others become resigned to it but – notwithstanding dogma – none ‘accept’ the bit. If it was not strapped in place, it would be spat out. As horses instinctively reject anything in the mouth other than food or water, this prompts the question – why signal with ‘metal-on-bone’ (provoking touch and pain receptors) when ‘strap-on-skin’ (touch only) can be painless? A bit-free signal, with none of the signal ‘noise’ caused by pain, is better understood by the horse and improves compliance. Accidents are less likely if ‘misunderstandings’ by the horse are avoided. A bitted-rein signal is overkill for an animal as sensitive as a horse. For a human comparison of the pain of ‘metal-on-bone’, think of the ‘bone-on-bone’ pain of severe arthritis. Sixty-nine behavioral signs of pain attributable to the bit have been identified to date (Cook and Kibler, 2018a); many more await confirmation – especially in the racehorse. The evidence tells us that if riders signal with metal in the mouth, they do so at their peril and generally to a horse’s discomfort.
Airway structure and function
To understand the abnormal, the normal must first be recognized, i.e., the horse in the wild. Hence, the naming of the parts follows and how these parts normally work (Fig. 6).
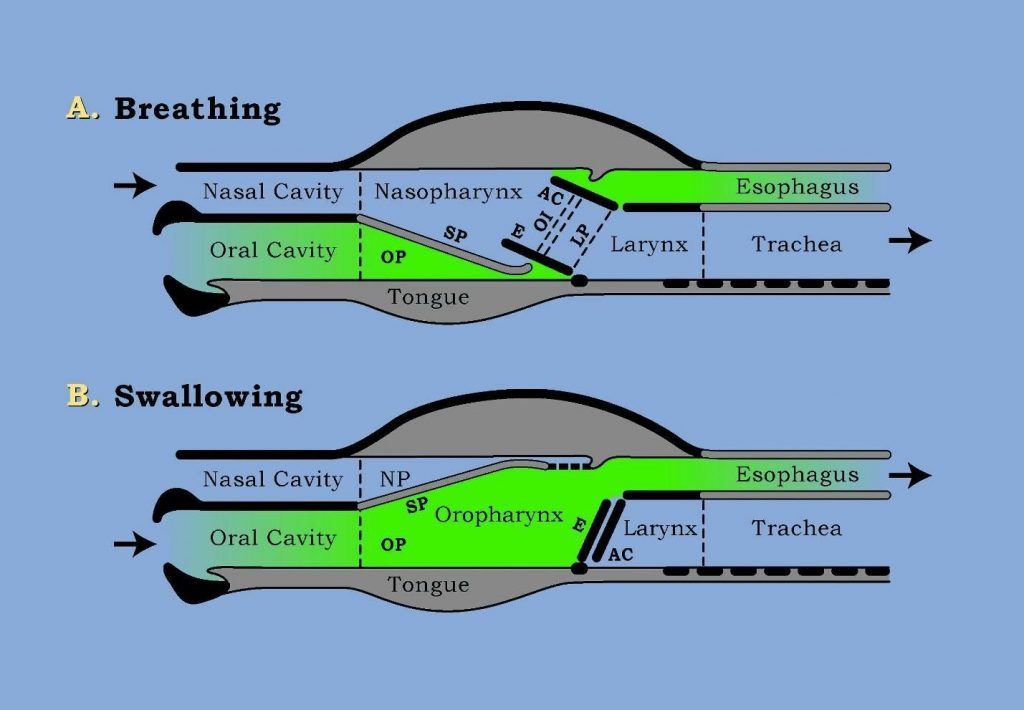
Key: AC = arytenoid cartilages; E = epiglottis; Larynx = voice-box; LP = laryngopharynx (the lateral food channels); NP = nasopharynx (respiratory part of throat); OI = ostium intrapharyngium (a ‘buttonhole’ in the soft palate); OP = oropharynx (digestive part of throat); SP = soft palate; Trachea = windpipe
Suffocation – upper airway
In addition to suffering pain, Mendelssohn in ‘Figure 1’ is suffocating from a combination of six factors:
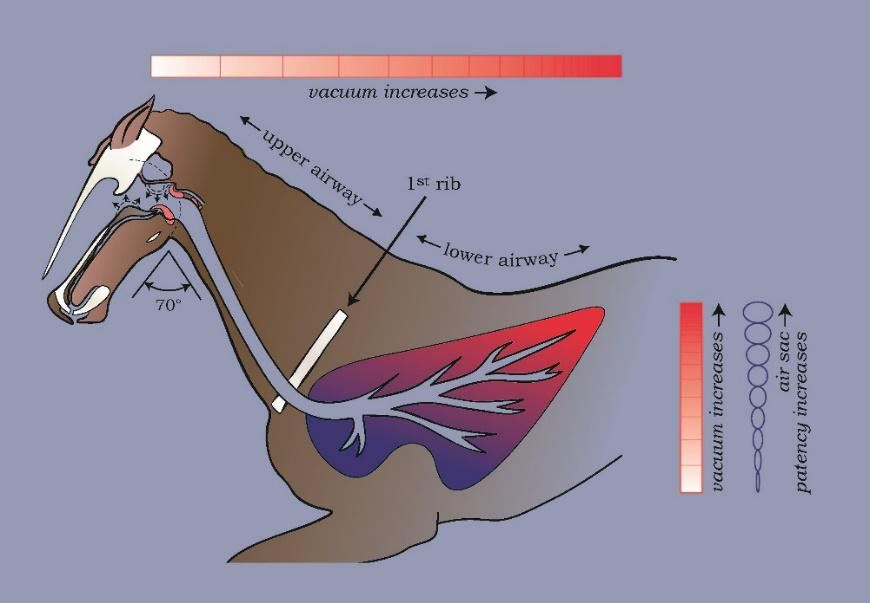
- Absence of poll extension: This will be increasing resistance to airflow and adds to the work of breathing. At the gallop, a horse needs to stretch-out to minimize airway kinks at the level of the throat and first rib.
- Open mouth: This will have dissipated what should, at exercise, be a sub-atmospheric pressure (partial vacuum) in the oral cavity and digestive part of the throat (red in Fig.7a). Mendelssohn’s long soft palate will be unstable. Equine evolution invented the principle of ‘vacuum packaging’ long before man used it to secure the lids of jam jars. Critically, a partial vacuum in the digestive part of the throat, initiated economically by just one swallow prior to running at liberty, stabilizes the horse’s soft palate on the immobile root of its tongue. In the wild, therefore, partial evacuation of air from the ‘digestive’ part of the throat serves to minimize its caliber and maximize the caliber of the ‘respiratory’ part of the throat which lies above it. In a bitted horse, the root of the tongue and the soft palate are likely to be mobile and the throat airway partially obstructed.
- Dynamic collapse of the airway, starting at the posterior nasal valves: The horse’s upper airway, from the back of the nose, through the throat, voice-box and windpipe to the first rib, can collapse in response to the negative pressure of inhaling. A soft palate that is not ‘locked-down on the root of the tongue’ at the gallop (Figs.7a and b) is liable to be elevated at each intake of breath by even a normal negative pressure during inhalation. The front part of the soft palate will act like a flapper valve and begin to obstruct both posterior nostrils. Once even this slight elevation is initiated, the negative pressure becomes stronger because of partial airway obstruction and a vicious cycle of dynamic collapse commences. This may result in complete dorsal displacement of the soft palate from the voice-box (Fig.7b) but also a cascade of collapse in other parts of the throat and, downstream, in successive parts of the upper airway, i.e., in the voice box and the long windpipe in the horse’s neck (Fig. 9). In my view, palatal instability and dorsal displacement of the soft palate are the cause of airway obstruction on inspiration, not as has been described in the past, on expiration. The position of the soft palate is key to understanding suffocation.
Key: red = regions partially evacuated of air by a pre-run swallow; broken line between nasal cavity and nasopharynx = posterior nostril (or choana from the Greek for funnel)
Nasal valve collapse is a well-recognized problem in human medicine, at the anterior nostril. A similar problem at the level of the muzzle can also occur in the horse, perhaps as a result of a bit-induced increase in respiratory effort. Airway obstruction at the horse’s posterior nostril (Figs.6, 7a and b, 8) is also a serious ‘nasal valve’ problem, caused by the bit, but one that has been overlooked. There is no equivalence between human nasal valve problems and those of the horse. In man, these are relatively uncommon, anterior nostril obstructions, and they generally occur on one side only. Though they can affect quality of life, they are not life-threatening because oral breathing is an option.

In the bitted racehorse, posterior nasal valve collapse is common, bilateral and potentially life-threatening because a horse cannot mouth-breathe. Simultaneous dynamic collapse of both posterior nasal valves, which undoubtedly occurs, cannot be seen endoscopically. With current endoscopy protocols, even unilateral collapse cannot be observed, as the endoscope lies in the valve, generally on the right side, so that the operator can view the posterior half of the throat and the voice box (Fig. 8).
Videoendoscopy footage available on YouTube shows what collapses are seen in the throat and voice box. Poiseuille’s law predicts (see below) that although these collapses can be caused by the bit and other problems, they can also be caused by the endoscope itself, which obstructs the major nasal airway on the side through which the endoscope is inserted (Fig 8). A second examination under similar conditions but without a bit and without poll flexion may help to rule-out endoscope -induced dynamic collapse from other causes but only if no collapses are present at the second examination.
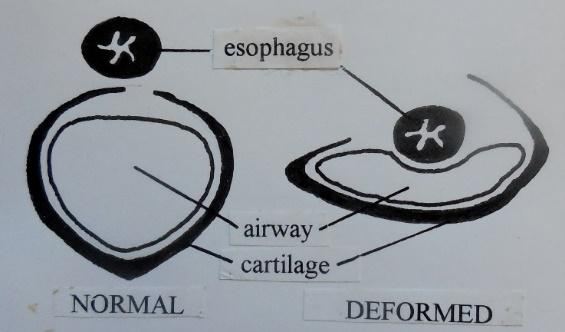
Dynamic collapse of the first ring of the windpipe has been reported but rarely. Subsequent rings are out of view endoscopically so, understandably, bit-induced dynamic collapse of the windpipe is not a feature of publications on videoendoscopy. However, Poiseuille’s law determines that, in the presence of an obstruction in the nasal or laryngeal section of the airway, successive rings of the windpipe in the neck will develop dynamic collapse during inhalation. Furthermore, the law predicts that the most severe collapse will occur (far out of sight endoscopically) in rings at the base of the neck (i.e., level of first rib). This inevitable feature of bit-induced suffocation makes bit-induced lung damage easier to understand. (see ‘Suffocation – lower airway’). Autopsy evidence provides tangible support for windpipe dynamic collapse having occurred at bitted exercise. My experience of autopsy studies of cross-sections of the windpipe supports the view that permanent deformities of the windpipe are common long-term effects of repeated episodes of dynamic collapse during bitted exercise. There are about 40 rings of cartilage in the neck section of a horse’s windpipe. A deformity in any one of the rings hinders airflow. The troubling reality is that all 40 rings are vulnerable to dynamic collapse and its sequel, permanent deformity (Fig. 9a). Again, in my experience, it is common for nearly all 40 rings in a racehorse to be deformed to varying degrees. This ‘scabbard’ type deformity is not a rare phenomenon limited to miniature horses and ponies.

- Rein tension: The ‘strong-hold’ of the reins will be restricting the range of the head/neck pendulum (‘head bob’); adding to the work of breathing (increasing respiratory effort), wasting energy, hastening fatigue.
- Retraction of the tongue: This will be causing the tongue’s root to bulge upwards, elevating the soft palate, diminishing the caliber of the throat airway (the ‘nasopharynx’ in Fig.7b). The tongue is a hydrostat, i.e., an organ of constant volume. When its length decreases, its height increases.
- ‘Shaking’ airway: The tongue-tie has failed to prevent retraction of the tip of the tongue and the pain caused will be inciting movement at the root of the tongue and the soft palate above it – the antithesis of ‘open-throated,’ closed-mouth breathing. Poiseuille’s law does not mention the effect on airflow of a ‘shaking’ tube but this is yet another factor incompatible with laminar airflow.
The root of the tongue and the voice box (i.e., the entrance to the windpipe, indicated by the ‘lung’ end of the double-ended arrow in Fig.7a) are anatomically connected. They are joined by bone scaffolding (hyoid apparatus) that suspends them both from the base of the skull. Any movement of tongue or jaw when running also moves the voice box, adding to turbulence of airflow already initiated in the throat.
Poiseuille’s law
Key to understanding the serious consequences of the above six factors is a law of physics governing the laminar flow of liquids and gases in tubes (fluid dynamics). Poiseuille’s law lists four governing factors, the radius and length of a straight tube, the viscosity of the liquid or gas, and its velocity (the speed of airflow). The law needs our close attention because it is of fundamental importance to racing.
- Radius: If the radius of a horse’s airway is halved, resistance to airflow increases by a factor of sixteen. Because resistance varies directly with the fourth power of the radius, any airway obstruction has to be of great significance for a sport in which success is measured in fractions of a second to two decimal points.
- Length: The functional harm of any airway obstruction is significantly dependent on its location within the airway. The closer it is to the ‘mouth’ of the tube, the more severely is lung function impaired. An obstruction at the ‘posterior’ nostril (Fig.7b) suffocates and seriously handicaps a racehorse. Because some episodes of suffocation may cause permanent lung damage, future racing potential may be also be jeopardized.
- Viscosity: The ‘thickness’ of the air we breathe varies with the ambient temperature of the air, its humidity and particle content. Higher viscosity increases laminar flow resistance. Mendelssohn may not have been negatively affected by the quality of air on the day of the photograph. But, because his airway was partially obstructed, as explained above, turbulent flow will have been initiated. This, by definition, increases the air’s viscosity, so increasing friction, i.e., resistance to airflow and the work of breathing.
- Velocity: Mendelssohn was only cantering but airway obstruction at any ground speed may cause the speed of airflow to switch from laminar flow (fast, easy, and economic in terms of ‘work’) to turbulent (slow, viscous and hard work, i.e., energy ‘expensive’). Airflow resistance and the work of breathing will thus be increased. Airway obstruction at racing speed will have many consequential effects, including rapid onset fatigue.
The implication of Poiseuille’s law is that, with any upper airway obstruction, we need to pay attention to what effect this obstruction has on increasing degrees of obstruction (suffocation) downstream in the windpipe and, ultimately, on the damage it causes to the lungs.
Airflow resistance is defined as the ratio of driving pressure to the rate of air flow (velocity).
Bits can bruise lungs. A decrease in the supply of air caused by an airway obstruction could be compensated for by an increase in demand, i.e., an increased respiratory effort (the work of breathing). But there is a limit to how far this can safely go. If a key driving force of breathing, the diaphragm, exerts too strong a force (too powerful a negative pressure in the chest) the lungs may become massively bruised (waterlogged), the heart may fail and death will follow. Alternatively, faced with an insufficient supply of air, a sense of drowning when the lungs begin to get waterlogged and start to ‘bleed’, a horse – perhaps experiencing chest pain – can reduce demand by decelerating, hence the much-lamented ‘poor performance.’ (Fig. 10).
All six forms of suffocation are relevant to racing in general. Any suffocation is incompatible with peak performance and puts the lives of both horse and rider at risk.
Suffocation – lower airway
The name for an air cell in the lung is alveolus; Latin for ‘small cavity’. One cubic millimeter of human lung contains around 170 alveoli. Think of each air cell as a microscopic, double-skinned, open-necked balloon immersed in a pool of capillary blood. Both ‘skins’ (inner ‘air’ skin and outer ‘blood’ skin) are membranous and very thin. The finest lace is bulky compared to the gossamer delicacy of air cells. Under normal (i.e., physiological) conditions, both skins are ‘porous’ to oxygen and carbon dioxide. The inner lining of the cell is in direct contact with outside air, just like the skin of the face. The difference is that whereas facial skin is
impermeable to gas and water, the ‘air’ and ‘blood’ skins of the alveoli are permeable to both. Under abnormal conditions (i.e., during the development of abnormally strong negative pressures arising from the forced intake of air against an obstructed upper airway), plasma and red blood cells get sucked into the air cells. Air cells of both lungs are bruised at each strangled breath. Two or three seriously obstructed breaths can quickly lead to a life-threatening condition in man called ‘negative pressure pulmonary edema or NPPE (‘waterlogging’ of the lung).
In the racehorse, the slightest obstruction to the intake of air lowers pressure in the air cells. I have proposed that it is the rapid onset of waterlogging of the lung that most commonly results in the all too familiar ‘sudden death’ of a racehorse. In man, severe NPPE is accompanied by chest pain and a sense of drowning, as in waterboarding.
In the horse, the condition currently named exercise-induced pulmonary hemorrhage or EIPH is defined as “bleeding that occurs from the lungs of horses during exercise” (Hinchcliff et al, 2015). In my view, limitation of the literature review by the panel of the American College of Veterinary Internal Medicine (ACVIM) to one sign (bleeding) and one circumstance (exercise) has led to the same type of misperception arrived at by the proverbial six blind men who each manually investigated different parts of the same elephant. They variously averred, each with confidence and all of them wrongly, that an elephant was ‘like’ a wall, spear, snake, tree, fan, and rope’, depending on which part of the elephant they explored.
As a result of investigating only one part of the equine veterinary ‘elephant’ (i.e., publications solely on EIPH) the seven members of the ACVIM panel concluded, unanimously, that EIPH was ‘like’a disease. To cite the consensus statement, the panel issued a “Strong recommendation that EIPH be considered a disease” and added that EIPH “adversely affects the health, welfare or both of horses.” I agree with the panel’s conclusion but regret that notably absent from the objectives the panel set themselves to review was the cause of EIPH. My hypothesis is that EIPH is caused by bit-induced suffocation. I further postulate that EIPH is a much larger ‘elephant’ than ‘bleeding and exercise.’ By taking into consideration a greater number of signs and circumstances, and their likely cause, I believe a more constructive conclusion is justified.
In my view, EIPH is only one part of a larger problem and is ‘like’ (the same as) the human disease NPPE. If EIPH were renamed NPPE, this would lead to a better understanding of the problem and its solution. Indisputably, the ‘elephant in the room’ of racing is ‘exercise and lung bleeding’ but it is also ‘extreme exercise, weight-carrying exercise, head-bob restricted exercise, unsealed lips, strangulation, shortage of air, pain, fear, fatigue, exhaustion, sprained tendons, torn ligaments, falls, fractures, dislocations and sudden death.’ I postulate that suffocation is a cause of catastrophic breakdowns. I believe suffocation can also, in turn cause asphyxia, i.e., heart failure and sudden death. Note, that although the words ‘suffocation’ and ‘asphyxia’ are usually used interchangeably, the etymological origin of the word ‘asphyxia’ is ‘a ceasing to throb’. Thus, strictly speaking, it is correct to say that suffocation can lead to asphyxia (heart failure) and sudden death. The suffocation hypothesis is testable, as it is vulnerable to refutation. As noted below, such rigorous testing has been recommended (Mellor and Beausoleil, 2017).
Apart from Mendelssohn’s situation at one photographic moment during a workout on one particular day, some circumstances that could affect every bit-burdened racehorse on any day are relevant:
Mechanism of breathing: Compared with the demand for oxygen when grazing, a horse in the wild needs additional oxygen when running. The increased demand is supplied in an elegant and economic fashion; the increased stride-rate automatically increases the respiratory-rate and depth of breathing. It could be said that a running horse breathes with its legs – one breath for every stride. This is true but only part of the story. In fact, the running horse uses the whole of its body to breathe at the gallop; its liver-weighted diaphragm, its legs, spine, head-and-neck. The unimpeded and pendulum-like swing of the ‘head bob’ (likely to be restrained in Mendelssohn’s case) is an energy-saving mechanism for both locomotion and respiration. Without it and, compounded by suffocation, premature fatigue (poor performance) is likely to occur. Because breathing and striding are linked, turbulent breathing will negatively affect striding, which is a major impediment for a racehorse.
Supply and demand: When ridden, the weight of the rider increases the demand for oxygen. Evolution is a parsimonious process. To avoid wasting resources on maintaining structural ‘strength’ surplus to that needed during naturally occurring emergencies (e.g., evasion of predators), evolutionary development does not build-in more capacity than necessary. At first glance, it might seem that the additional demand for oxygen consequent on carrying weight (the jockey) could not be met – except that evolution has allowed for a full-term pregnant mare to gallop. Nevertheless, demand for oxygen may still exceed supply when a ridden and bitted horse is required to gallop beyond its natural flight distance of about two furlongs.
Behavioral changes: Direct effects of oral pain and other bit-induced factors degrade the function of bodily systems, which may lead to suffocation and its effects such as fatigue, chest pain, fear and panic. Also, longer-term effects, such as ‘hair-trigger’ shying (spooking) and other accident-inducing changes of character, caused by chronic emotional stress, may lead horses to become uncooperative, argumentative and even aggressive.
Reined-in riding: Poiseuille’s law refers to laminar flow in straight tubes but bends in a tube also potentially threaten laminar flow. In a one-furlong workout at a stride-rate of 120 strides/min, a horse will take about 24 breaths. If Mendelssohn cantered even only half a furlong, 12 obstructed breaths through a twice-kinked airway would probably be enough to cause some ‘waterlogging’ of the lung. Whether this occurred is unknown but, predicted by Poiseuille’s law even for an obstructed straight airway it is a possibility A horse ‘reined-in’ during a workout 24 hours prior to a race may be at risk of starting the next day with a sore mouth and impaired lungs. Any lung damage incurred will be additional to any long-term damage (e.g., inflammatory airway disease) similarly accumulated since training first commenced.
Racehorses are bitted and most are reined-in for some sections of most races. In my view, it is not a coincidence that most racehorses bleed from the lungs and some die. Shortage of air leads to muscle weakness and premature fatigue in any athlete. It seems reasonable to propose that suffocation in the racehorse may be a cause of poor performance and a factor in the cause of tendon strains, falls, fractures and dislocations.
Part II: The Solution
The evidence suggests that a bit-free racehorse would have sealed lips and would not experience pain in the mouth or a ‘tight’ chest. Bitted horses that bolt because they are experiencing bit-induced pain/panic are understandably unresponsive to any further rein-aid signals. In contrast, a bit-free horse will respond willingly to a painless rein-aid signal to slow down, a signal which is based on touch alone and transmitted to a small area of facial skin; i.e., the chin and, to a lesser extent, the bridge of the nose (Fridtjof Hanson 2019: Personal communication). A signal for deceleration should not include pain and, indeed, pain is contraindicated. Bit-free racing is possible, practical, and preferable (Fig. 11). Racehorses can ‘be given’ their head. It is my prediction that a bit-free racehorse would not ‘bleed’ and would be at reduced risk of catastrophic breakdowns. Other likely benefits would be improved steering, performance, and the public relation’s image of racing – thereby helping to sustain the sport’s social licence.

Breeders, owners, and trainers could:
- Teach foals to lead in hand and respond to the lightest of lead-shank signals.
- Train yearlings under saddle, bit-free from the start.
- Train two-year-olds on a bit-free rein but, while mandatory bit rules apply, accustom horses to the presence of an inactive (‘dummy’) bit in the mouth.
- Race them with two pairs of reins, one bit-free rein (active) and one dummy-bit rein (inactive). Alternatively, use a single rein to a bit-free bridle that is also attached to a dummy bit but so adjusted that no tension is applied to the dummy.
By training a racehorse – essentially bit-free – much could be accomplished.
- Horses will exhibit, by their behavior, a willing compliance to respond to a pain-free rein.
- Exercise-riders and jockeys will be reassured and become confident that a pain-free rein provides enhanced communication and safety
- Stewards of racing will have the opportunity to observe health, welfare and safety advances.
- Training injuries and accidents will be reduced.
Though the ideal is to avoid hurting, frightening, or suffocating a horse in the first instance, horses that have already been trained using a bit can be beneficially transitioned to being bit-free. Horses are quick learners when not in pain.
Racing’s administrators will need time to consider the above evidence. By allowing bit-free training on training tracks under their jurisdiction, racing’s stewards would be able to witness first-hand that bit-free racing will not result in the accidents they fear; quite the opposite.
In their thorough review of the literature on breathing in the horse, two animal welfare scientists conclude that “there is the potential for ridden horses to experience three forms of breathlessness – “unpleasant respiratory effort”, “air hunger” and “chest tightness” – which arise when there is a mismatch between a heightened ventilatory drive and the adequacy of the respiratory response” (Mellor and Beausoleil, 2017). They recommend that studies be undertaken to compare oxygen levels and other respiratory markers, when bitted and bit-free, to evaluate the likelihood of bit-induced breathlessness in horses. In the meantime they observe that “most horses exhibit clear behavioural evidence of aversion to a bit in their mouths, varying from the bit being a mild irritant to very painful. This in itself is a significant animal welfare issue that should be addressed.”
As judged by videoendoscopy and other studies, bitted horses often exhibit abnormally low levels of oxygen in their blood after exercise (hypoxemia). When the recommended bit vs bit-free studies are conducted, videoendoscopy should not be part of the experimental protocol because, as determined by Poiseuille’s law, the endoscope itself (Fig. 8) constitutes an upper airway obstruction (Cook 2018c)
Conclusion
Aside from the health and safety risk to horse and rider in using a bit, the practice raises the question of whether it is ethically justifiable to cause a horse pain for racing or any sport. The practice also raises a paradox. Bit usage runs counter to the principal reason why owners keep racehorses in training – to win races. By using a bit for a discipline requiring peak performance, a horse’s demand for air is likely to exceed supply. Bits can cause both pain and breathlessness. In the absence of any evidence to refute this statement, rules mandating use of a bit subvert the sport’s main purpose.
Acknowledgements: The article is dedicated to my wife, Margaret, who lived 93 loving years. For gently guiding the article editorially through many drafts, I am deeply indebted to Professor Emeritus, David Mellor. For the generous use of two copyrighted photographs, I thank Eric Kalet and Emma Preikschat
Further Reading
(In publication date order)
Gebiss-Debatte (2018): Was macht das Gebiss mit Pferden? Cavallo 11 November 2018, pp16- 35
Cook W.R. (2018a): What does a bit do to a horse and rider?
Cook W.R. (2018b): Seventy reasons for not using a bit. The Horse’s Hoof, July issue, pp 26-29. https://www.horsetalk.co.nz/2018/07/03/70-reasons-for-not-using-a-bit/
Cook W.R (2018c): Fifty years of recurring struggles with recurrent laryngeal neuropathy. Equine Veterinary Journal. 21 July 2018,
Cook W.R. and Kibler, M. (2018): Behavioural assessment of pain in 66 horses, with and without a bit. Equine Veterinary Education. Open access (free) article available at https://doi.org/10.1111/eve.12916 and for non-veterinarians at
Mellor, D.J and Beausoleil, N.J. (2017). Equine welfare during exercise: An evaluation of breathing, breathlessness and bridles. Animals 7, 41; doi:10.3390/ani7060041 (open access article) at
http://www.mdpi.com/2076-2615/7/6/41 and for non-veterinarians at
Cook, W.R (2016): Bit‐induced asphyxia in the racehorse as a cause of sudden death. Equine veterinary Education, 28,405-409
Hinchcliff, K.W, Couetil, L.L, Knight, P.K, Morley,P.S, Robinson,N.E, Sweeney, C.R, and van Erck.E (2015): Exercise Induced Pulmonary Hemorrhage in Horses: American College of Veterinary Internal Medicine Consensus Statement. Journal of Veterinary Internal Medicine, 29:743–758
Cook, W.R. (2014b): A hypothetical etiological relationship between the horse’s bit, nasopharyngeal asphyxia and negative pressure pulmonary oedema. Equine Veterinary Education, 26, 381‐389
Cook, W.R (2010): Damage by the bit to the equine interdental space and second lower premolar. Equine Veterinary Education, 23, 355-360 https://doi.org/10.1111/j.2042-3292.2010.00167.x+
")













")
